PAST HISTORY:
No similar complaints in past.
He is known case of diabetes and Hypertension since one year and was on regular medication.
No H/o Tuberculosis, Epilepsy,Asthma.
PERSONAL HISTORY:
Diet - Mixed
Appetite -Normal
Bowel and bladder -Regular.
Sleep - Adequate
Addictions: consumes Alcohol since 40 years and Smoker consumes 3 to 4 biddi per day.
FAMILY HISTORY:
No signicant Family history
GENERAL EXAMINATION:
Patient is conscious ,coherent ,cooperative
He is moderately built and nourished.
Pallor - Absent
Icterus - Absent
Cyanosis - Absent
Clubbing -present
lymphadenopathy - absent
Pedal edema - absent
Vitals : on the day of admission
Temperature - Afebrile
Pulse rate - 103 bpm
Respiratory rate - 16 cpm
BP- 180/90 mmHg
SpO2 - 96% on Room air
GRBS - 160mg/dl
SYSTEMIC EXAMINATION:
CNS Examination:
Face is turned towards Right side.
-Loss of speech
Cranial nerves :
CN 7- nasolabial fold on left side is less prominent. Deviation of mouth to Right side. Forehead wrinkles are absent on left side.
CN 11-Sternocleidomastod muscle spasm on right side.
Other cranial nerves are normal.
ATTITUDE:
Left upper limb - flexed and pronated
Left lower limb - externally rotated
BULK of the muscles - Normal
POWER : Right Left
Upper Limb 4/5 0/5
Lower Limb 5/5 0/5
TONE : RIGHT LEFT
UL NORMAL CLASP KNIFE
LL NORMAL HYPOTONIA
REFLEXES : Right side. Left side.
Biceps Present Absent
Triceps Present Absent.
Supinator Present. Absent.
Knee Present. Absent
Ankle Present. Absent
CVS :S1 ,S2 heard , no murmurs.
RESPIRATORY SYSTEM:BAE Present.
PER ABDOMEN::
Soft and non tender , bowel sounds +
CLINICAL IMAGES:




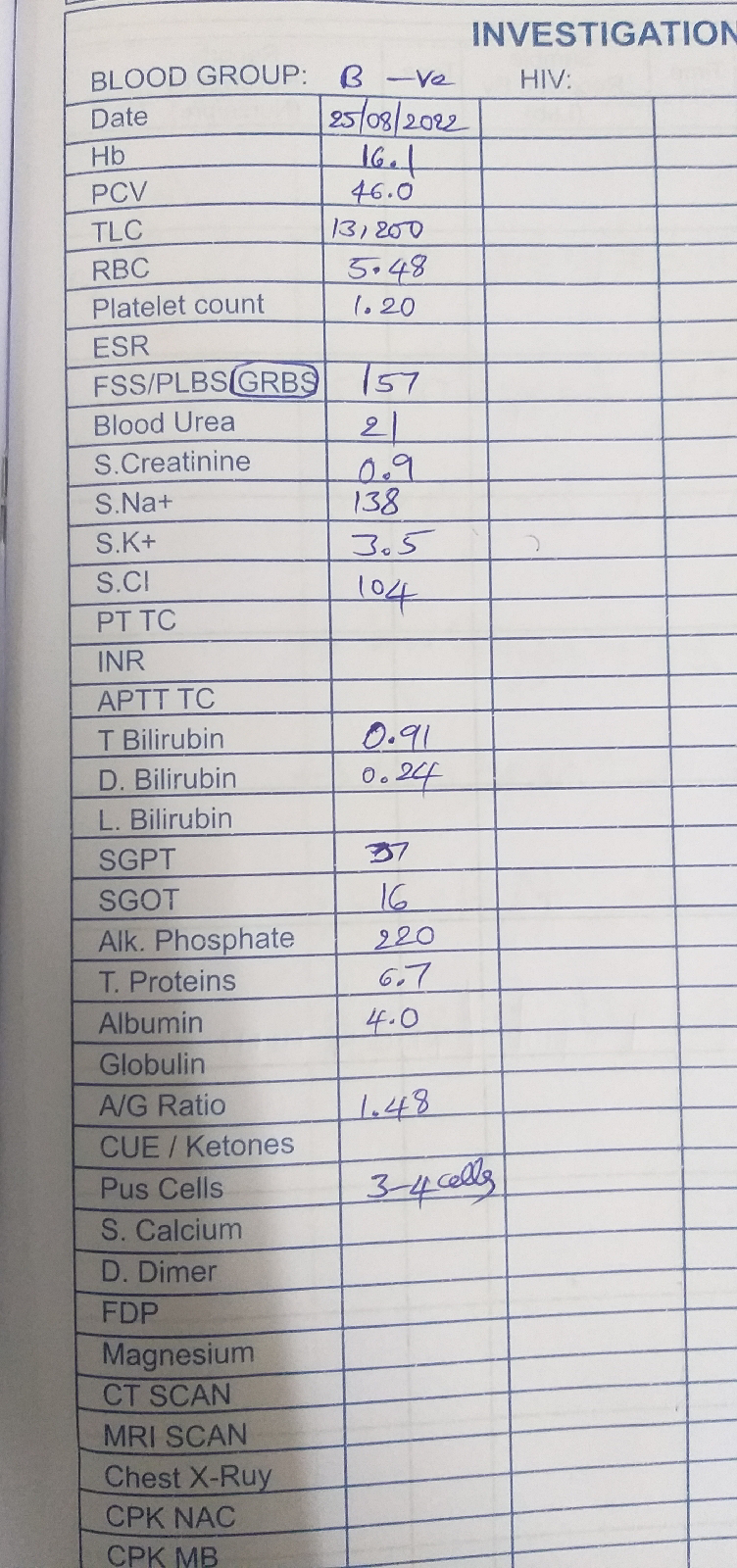
Investigations:








{kind=link}
No comments:
Post a Comment